
Adult Lower Leg Fractures
|
||||||


Introduction
Physical therapy in Seattle for Lower Leg Fractures
Welcome to Core Physical Therapy’s guide to lower leg fractures.
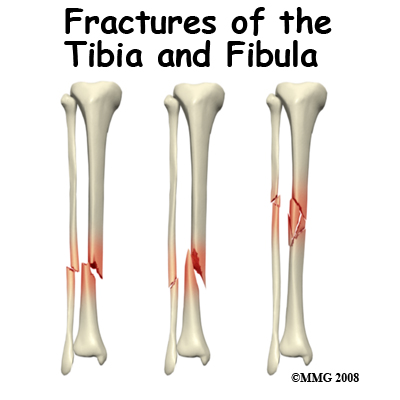
In this guide we are concerned with fractures of the lower leg between the knee and ankle. The two bones in the lower leg are the tibia and fibula. We will limit this discussion to fractures of the shaft, or mid section of these two bones. Fractures of the lower end of the tibia and fibula are covered in ankle fractures. Fractures of the upper end of the tibia are covered in knee fractures.The tibia bone is the largest and most important bone of the lower leg. It is quite vulnerable to injury. There is no overlying muscle to cushion impact on the front and inner side of the bone. The tibia is relatively easy to fracture with twisting or bending forces. As a result, fracture of the tibia is one of the most common major long bone fractures encountered in adults. Fracture of the tibia has a reputation for complications including failure to heal, or nonunion, so the management of this injury needs a careful approach from orthopaedic surgeons.
Usually, when the shaft of the tibia is broken the fibula, the smaller bone of the lower leg, is broken as well. This bone serves mainly as an anchor point for muscle and hardly bears any weight. As a result it does not need to be perfectly straight when it heals. It is sometimes surprising to patients that the doctors pay so much attention to the tibia and so little to the fibula.
This guide will help you understand:
- what parts of the lower leg are involved
- what the symptoms are
- what can cause these fractures
- how health care professionals diagnose these fractures
- what the treatment options are
- the Core Physical Therapy’s approach to rehabilitation
#testimonialslist|kind:all|display:slider|orderby:type|filter_utags_names:Foot therapy|limit:15|heading:Hear from some of our *Foot Therapy* patients#
Anatomy
What structures are most commonly injured?
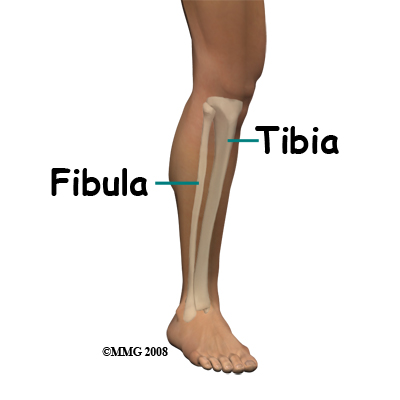
The tibia is shaped a little like an inverted trumpet with a long straight shaft flaring out at the knee. The shaft has a triangular shaped cross-section and the inner front portion of the bone has only skin overlying it. If you put your finger on the inner side of the knee and run it down all the way to the inside of the ankle you can feel bone all the way down.
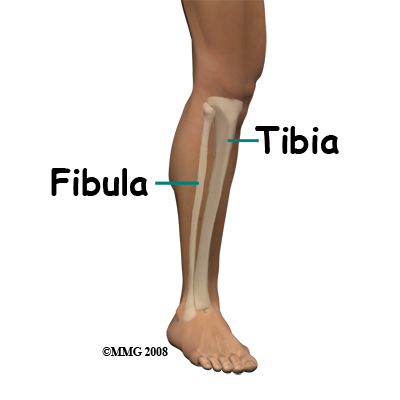
There are muscles surrounding the tibia on the outer side and at the back; the fibula is completely surrounded. Because the bone is just under the skin it is quite common for the jagged end of the bone to come through the skin when it breaks, causing an open fracture. Fractures occur almost anywhere along the shaft of the tibia but the most common site is about two thirds the way down.
The blood vessels and nerves that supply the foot are quite close to the bone. It is not uncommon for fractures of the shin, especially open fractures to involve damage to either the blood supply to the foot or the nerve supply or both.
Related Document: Core Physical Therapy's Guide to Ankle Anatomy
Related Document: Core Physical Therapy's Guide to Knee Anatomy
Causes
How do fractures of the lower leg commonly happen?
The tibia and fibula can be broken by a number of different forces, impact against the leg, compression, bending forces or twisting forces. It is possible to break the fibula in isolation, without fracturing the tibia, although this is an uncommon situation caused by a direct blow to the outer side of the leg. Isolated fracture of the tibia is slightly more common but usually both bones break.
It is important to remember that whenever bones are broken there is also damage to muscle, tendon, ligament and often nerves and skin. This soft tissue injury does not show on X-ray but it contributes greatly to the pain and swelling of the injury - and may affect the eventual outcome.
Types
What Types of fractures can occur?
The different patterns of fracture of the tibia and fibula relate to the different mechanisms of injury. Oblique fractures are usually caused by a bending force or direct impact. Transverse fractures result from compression and spiral fractures result from twisting forces.
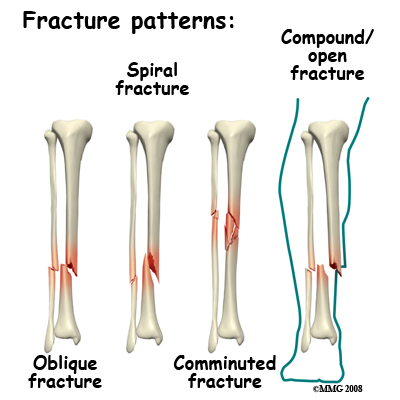
The more force applied; the more likely it is that there will be multiple fragments. The term used to describe multiple fragments is comminution; a fracture of this type is referred to as a comminuted fracture. It is also more likely that the displacement of the fracture fragments by the greater force will push one or more of them out through the skin, causing an open fracture.
Fractures of the tibia are common in high energy accidents such as MVAs or falling from a height. The leg may get caught in machinery causing severe fractures with extensive skin loss and potential for major injuries to muscle, tendons, nerves and arteries. Sports such as skiing, contact sports and tobogganing all cause their share of leg fractures. Falls in the elderly do sometimes cause fractures of the shin bone; in these cases the fractures should be considered fragility fractures. Pathological fractures through abnormal deposits in bone occur rarely.
Symptoms
What symptoms do lower leg fractures cause?
People who suffer a fracture of the tibia and fibula have immediate pain at the site of the fracture. The pain is made worse by any movement of the limb. Often the leg is deformed, either twisted or bent, and sometimes there is a wound where the bone has come out through the skin.
In the case of an isolated fracture of the fibula you may be able to walk, but with nearly all other fractures it is impossible to bear weight. Within a few minutes of the injury the leg will swell up. If there have been injuries to the nerves or arteries the foot may be numb or cold.
Within hours of the injury there will be significant bruising. Fracture blisters are seen quite often after fractures of the tibia. Pain, swelling and bruising are evident for weeks after a break regardless of the treatment. This is because of the soft tissue injury, bleeding into the muscle compartments, and compromised circulation in the injured area. The worse the soft tissue injury the more likelihood there is of stiffness or weakness of the nearby knee and ankle joints.
Aching discomfort in the affected area and some pain on stressing it may continue for many months while the fracture is healing and consolidating. It should gradually diminish as the fracture heals and regains normal strength. Where metal implants have been used to treat the fracture, tenderness, mild aching, and cold intolerance may persist until the implants are removed.
Evaluation
How will my fracture be evaluated?
First aid treatment at the scene of the accident should consist of keeping the victim warm, splinting the leg, and transporting him/her to hospital. An assessment at the scene should include dressing any wounds and checking for numbness of the foot. It is not usually necessary to straighten the leg unless it cannot be splinted otherwise.
In the Emergency Room the focus is on treating shock, making the patient comfortable, ruling out other injuries, and getting the correct x-rays to evaluate the fracture. It is important to obtain x-rays that include the ankle and knee. If an isolated fracture of the shaft of the fibula is diagnosed this may be treated by the emergency doctor and followed by your family doctor. Fractures of the shaft of the tibia usually result in referral to an orthopaedic surgeon.
The orthopaedic assessment may include an evaluation of the general medical status of the patient and the risks of anesthesia. The history of the accident and the forces causing the fracture will be assessed and the limb carefully examined for wounds, blistering, skin problems, neurological or vascular loss and for signs of injury to the knee or ankle. The X-rays will be reviewed and more X-rays obtained if necessary.
The treatment plan will be discussed with the patient giving consideration to the nature of the fracture, the patient's health status, level of activity, occupation and expectations. The most important feature of the fracture is whether it is stable or not. An unstable fracture is likely to shorten, angulate or rotate and may need treatment with surgery.
Our Treatment
What treatments should I consider?
An isolated fracture of the fibula may be treated in a cast for protection or may be left alone. The bone will heal without interference and the aims of treatment are to manage the pain. Using crutches for a few weeks is usually recommended.
The treatment of fractures of the tibia is controversial. Some orthopaedic surgeons take the view that most such fractures should be treated by operation. This is supported by scientific studies that show with surgery the fracture healed more reliably and with better alignment. Others prefer to avoid an operation unless it is clear that the outcome will be poor without surgery.
There is also controversy about the type of operation best suited to this injury. There is such variation in the patterns of injury and treatment that research studies to answer some of these questions are very difficult to organize. Most orthopaedic surgeons would agree that treatment has to be individualized and matched to the patient's injury pattern, medical status and expectations.
Nonsurgical Treatment

Treatment in a cast may be recommended when the fracture pattern is stable, there are no other major injuries and the patient is fit enough to carry the weight of a cast around. The pattern of injury most suited to cast treatment is a spiral fracture because it is inherently stable. Transverse fractures are also relatively stable. Oblique fractures are inherently unstable and likely to shorten. However, the amount of shortening is unpredictable and may be acceptable.
It is not unusual to begin treatment with a cast and then change course. In order to avoid an operation, cast treatment may be started initially and surgery later recommended if the bone fragments move and the position becomes unacceptable.
In some situations the cast can be applied without an anesthetic. The lower leg is hung over the side of the bed so that gravity keeps it straight. The cast is applied from toes to knee in this position and this splints the fracture in the reduced (straight) position. Then the leg is lifted onto the bed and the cast is continued up above the knee to form a long leg cast. The knee is bent about 40 degrees in the cast to prevent rotation and allow the leg to swing through during crutch walking.
Quite often it would be too painful to apply a cast without a general or regional anesthetic. The procedure is then done in the OR, the fracture is manipulated into a good position and the long leg cast applied. X-rays may be taken at this stage to confirm that the fracture is in a good position. If it is not, further manipulation may be undertaken or the surgeon may decide to operate. The option to continue on to an operation if closed treatment is not acceptable would be discussed with the patient ahead of time.
Once the cast has been applied it may be split to allow the leg swelling to occur without undue compression of the tissues. As the swelling goes down the cast may become loose and need to be tightened or replaced. Follow-up in the cast clinic at frequent intervals is usually recommended. X-rays will be taken to confirm good position of the fracture and assess healing as it takes place.
 If the fracture has moved, it may be possible to correct the position by wedging the cast. This involves cutting the cast three-fourths the way around at the level of the fracture leaving a hinge of intact cast on the convex side of the deformity. The leg can then be straightened and a wedge inserted into the opening in the cast on the concave side to hold the cast - and the bones - in the new position. Once x-rays have confirmed that the new position is acceptable, more plaster is applied over the cast to make it rigid once again.
If the fracture has moved, it may be possible to correct the position by wedging the cast. This involves cutting the cast three-fourths the way around at the level of the fracture leaving a hinge of intact cast on the convex side of the deformity. The leg can then be straightened and a wedge inserted into the opening in the cast on the concave side to hold the cast - and the bones - in the new position. Once x-rays have confirmed that the new position is acceptable, more plaster is applied over the cast to make it rigid once again.
Casting material is either plaster of Paris (POP) or some form of fiberglass. POP is cheaper and easier for the surgeon to work with, molding the cast to the shape of the leg. Fiberglass is lighter and more durable. Unlike POP is doesn't disintegrate if it becomes wet. However, if it does get wet the soggy padding may cause skin problems. It is better to keep any cast dry.
Casts are normally changed after six weeks. If there is x-ray evidence of healing the surgeon may select a shorter, patellar tendon bearing cast or brace and allow some weight bearing. It is normal for some form of splinting to continue for at least three months. The length of time the fracture needs to be protected by a cast or brace depends on the amount of healing. There is a risk of re-fracture until full healing of the fracture has been achieved. So, there is no "normal" length of time to be in a cast after a tibia fracture.
Surgery
All open fractures need surgery to clean up and irrigate the wound. It does not follow that the fracture should be treated surgically as well as the wound. However, in many cases cleansing the wound is followed by fixing the fracture. It is believed on the one hand that an immobile fracture is less likely to get infected and is easier to treat if it does; on the other, surgery disturbs the blood supply and increases the exposure of the bone to contaminants so may increase the risk of infection. A compromise approach is to delay definitive fixation of the fracture until the open fracture wound has started to heal. Either way, an open fracture is a compelling reason for surgery on the wound.
Surgery on the fracture may consist of open reduction and internal fixation with a plate, closed reduction and fixation with an intramedullary rod, or reduction and external fixation. The fundamental reason for undertaking surgery is the surgeon's opinion that the result of surgery would be better than the outcome following cast treatment. In this context "better" means healing faster, stronger, in better position with less complications with quicker return to normal function.
Open Reduction and Internal Fixation (ORIF)
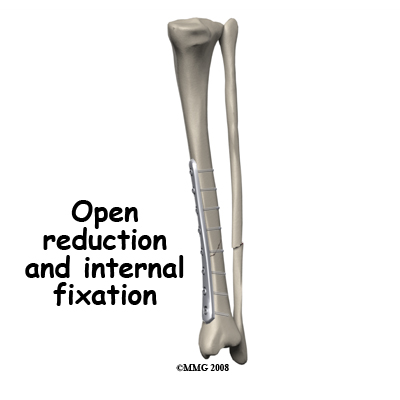 The operation involves exposing the fracture and moving the fragments back into the correct position. This position is then held by a metal plate secured above and below the fracture with screws. Plates are now available which match the shape of the tibia almost exactly. This allows a minimally invasive approach to plating the tibia where the plate is introduced under the skin.
The operation involves exposing the fracture and moving the fragments back into the correct position. This position is then held by a metal plate secured above and below the fracture with screws. Plates are now available which match the shape of the tibia almost exactly. This allows a minimally invasive approach to plating the tibia where the plate is introduced under the skin.
Intramedullary Rod Fixation
In this procedure the fracture is straightened (reduced), a small hole is made in the bone just below the knee and a guide wire is passed across the fracture inside the bone. A reamer is often used to make sure the fit is tight. Then a rod is slid into the hole inside the bone from the top. It is passed over the guide wire and into the lower fragment. To prevent the fracture shortening the bone is secured to the rod with transverse (locking) screws. The big advantage of this technique is that the fixation is very strong.
External Fixation
The bone is held in the correct alignment and length using a frame outside the leg. This is attached to the bone with transfixing pins or screws. This technique allows access to the wound, it is minimally invasive preserving the blood supply and it can adjusted later to correct any deformity. External fixation is more commonly used with more severe open injuries and very unstable fractures.
After the surgery a splint may be used for pain relief. However, there is no need for prolonged cast immobilization of the fracture - the metal hardware holds it still. In most cases the wound is dressed and movement of the foot, ankle and knee is encouraged. Weight bearing through a fracture treated with surgery is not usually recommended until x-rays show there are signs of healing (six weeks).
Hardware Removal
After the fracture has healed the metal implants may cause minor symptoms. Plate and screw areas may be tender; more rarely the hardware irritates tendons that should move over the bone. In some people there is a dull constant ache and cold intolerance. If these symptoms become significant enough, the hardware can be removed. This is a relatively simple operation but the issue of hardware removal causes many patients a lot of concern.
It is often uncertain what the benefits of hardware removal surgery will be. People are concerned that the bone will be weakened and re-fracture or that they will experience discomfort as bad as the pain they had after the original surgery. Hardware removal does require an operation to expose the plate or the rod but the incidence of re-fracture of the tibia is low and the pain after surgery is less severe and short lived. The long-term results of hardware removal have been studied and shown to be very satisfactory with few problems and a high rate of satisfaction.
How long does it take to heal?
There is no "typical" fracture of the tibia and recovery depends to a large extent on the severity of the original injury. Clearly the outcome expected from a stable closed spiral fracture will be different from the result after the leg has been mangled in machinery.
The normal healing times are six weeks to achieve 50 percent of eventual strength, three months to reach 80 percent of eventual strength, and 18 months to complete the process of consolidation and remodeling of the fracture. If this is the only injury this time scale usually suggests change to weight bearing with some protection at six weeks (e.g., walking cast); unrestricted weight bearing and gradual return to sports or heavy working activities at three months; and consideration of hardware removal after 18 months.
Rehabilitation
If you have been immobilized, rehabilitation with a physical therapist at Core Physical Therapy will begin once the brace or cast is removed. Prior to this, simple toe wiggling exercises will be your only exercise. In cases where your full cast has been replaced by a patellar tendon bearing cast/brace (which allows knee motion) then it is important to also maintain knee range of motion even if you are not able to weight bear through that leg.
If you have had surgery to fixate your lower leg fracture, then rehabilitation at Core Physical Therapy will begin as soon as your surgeon recommends it. Sometimes therapy will be recommended even before you are allowed to fully weight bear. In other cases, rehabilitation will not be recommended until full weight bearing begins. Each surgeon will set his own specific restrictions based on the type of fracture, surgical procedure used, personal experience, and whether the fracture is healing as
expected.
Even if physical therapy for the injured leg has not yet begun, at Core Physical Therapy we highly recommend maintaining the rest of your body’s fitness with regular exercise. You can use an upper body bike if you are non-weight bearing or a stationary bike once weight bearing is allowed. If the surgeon fits you with a brace that allows you to take partial weight through your leg (i.e. walking cast) then you can even use a stationary bike while wearing it. Weights for the upper extremities and other leg are also strongly encouraged. Your physical therapist can provide a program for you to maintain your general fitness while you recover from your fracture.
If you are using crutches, your physical therapist will ensure you are using them safely and confidently and that you are abiding by your weight bearing restrictions. We will also ensure that you can safely use them on stairs. If you are no longer using crutches, your physical therapist will assist with gait re-education. Until you are able to walk without a significant limp, we recommend that you continue to use your crutches, or at least one crutch or a cane/walking stick. Improper gait can lead to a host of other pains in the knee; hip and back so it is prudent to use a walking aid until near normal walking can be achieved. Your physical therapist will advise you regarding the appropriate time for you to be walking without any support at all.
When the initial cast or brace is removed, patients may experience pain when they start to move their ankle joint or bear weight through the lower leg. This pain is from not using the joints regularly while you were immobilized, or it may be from concurrent soft tissue injury that occurred when you fractured your leg. Your physical therapist will focus initially on relieving your pain. We may use modalities such as heat, ice, ultrasound, or electrical current to assist with decreasing any pain or swelling you have around the fracture site or anywhere down the extremity. In addition, our physical therapist may massage the leg and ankle to improve circulation and assist with the pain.
The next part of your treatment will focus on regaining the range of motion and strength in your ankle, foot, and entire lower limb. Your extremity will look and feel quite weak and atrophied after the period of immobilization. Your physical therapist will prescribe a series of stretching and strengthening exercises that you will practice in the clinic and also learn to do as part of your home exercise program. These exercises may include stationary cycling and the use of theraband to provide some resistance for your lower leg. We may even give you exercises for areas such as your hip or back as these areas help to support the lower limb when you are weight bearing. If necessary your physical therapist will mobilize your joints. This hands-on technique encourages the stiff joints of your ankle, foot, and lower leg to move gradually into their normal range of motion. Fortunately, the initial phases of gaining range of motion and strength after a lower limb fracture go quickly. You will notice improvements in the functioning of your limb even after just a few treatments with your Core Physical Therapy physical therapist. As your range of motion and strength improve, we will advance your exercises to ensure your rehabilitation is progressing as quickly as your body allows.
As a result of any injury, the receptors in your joints and ligaments that assist with balance and proprioception (the ability to know where your body is without looking at it) decline in function. A period of immobility and reduced weight bearing will add to this decline. Your physical therapist will also prescribe exercises for you to regain this balance and proprioception. This might include exercises such as standing on one foot or balancing with both feet on an unstable surface such as a wobbly board or a soft plastic disc. Advanced exercises will include agility type exercises such as hopping or moving side to side. Eventually we will encourage exercises that mimic the quick motions of the sports or activities that you enjoy participating in.
Generally, the strength and stiffness one experiences after a lower limb fracture responds very well to the physical therapy we provide at Core Physical Therapy. With our initial one-on-one physical therapy treatment along with the exercises of your home program, the strength, range of motion, and proprioception gradually improve towards near full recovery/function over a period of 3-6 months even though the actual final stages of bone healing won’t occur for another 6-12 months after that. If your pain continues longer than it should or therapy is not progressing as your Core Physical Therapy physical therapist would expect, we will ask you to follow-up with your surgeon to confirm that the fracture site is tolerating the rehabilitation well and ensure that there are no hardware issues that may be impeding your recovery.
Core Physical Therapy provides services for physical therapy in Seattle.
Complications
What are the potential complications of this fracture?
Stiffness
This consequence of the treatment of a fracture of the tibia makes it clear that the process can sometimes take a long time. Not using the muscles and joints for an extended period can result in deterioration and an increased risk of posttraumatic osteoarthritis of the knee or ankle. This was more common when long leg casts were used for extended periods. The injury itself does not damage the joints (although the muscles may certainly be injured) so early mobilization is effective in preventing this complication. In order to prevent this complication an exercise program as outlined in the Rehabilitation section is needed once the bone is healed strongly enough to withstand stress.
Fat Embolism Syndrome (FES)
This rare but serious condition can occur after about one in fifty tibial fractures. Fat globules from the bone marrow enter the blood circulation via damaged vessels and pass to the lungs and brain. Under certain conditions this sets up an inflammatory response compromising lung function and clouding consciousness. Often the first sign is confusion, followed by respiratory problems. The condition itself is short lived and self-limiting but the patient may need intensive care, including ventilator support, in the short term. Formerly, this rare condition was fatal in 10 percent of FES cases; with early recognition and aggressive supporting treatment this figure is now much less. However, it does remain one of the few complications of otherwise straightforward fractures that can provoke an emergency.
Infection
Open fractures are common tibial injuries and have an increased risk of infection because the bone comes through the skin and is contaminated at the scene of the accident. Surgical site infections can also occur when a fracture is operated on. This means that infections caused by bacteria are seen in a number of patients with tibial fractures (two to five percent). Most patients who have an open fracture or an operation receive antibiotics to reduce the chance of this complication. An infection is suspected when the wound remains red, tender, and swollen longer than normal. If it breaks open, if pus drains from the wound, or if bacteria are cultured from the wound, the diagnosis is confirmed.
High doses of antibiotics are given intravenously and in most cases the wound is opened to clean out dead and infected tissue and prevent pressure build up. In some situations, beads containing antibiotics are placed in the wound for a few days to achieve high local levels of the medication.
Fixation of the fracture is usually maintained until the fracture is healed. Then the implants may be removed because cracks or scratches on the surface may harbor bacteria.
The aim of treatment is to heal the infection and the fracture. Established bone infection may be very difficult to eliminate and may cause failure of healing. Most often the measures taken to treat the infection do result in healing the fracture and eliminating the infection. It is undeniable, however, that an infection results in a lot more trouble and usually some additional surgery.
Compartment Syndrome
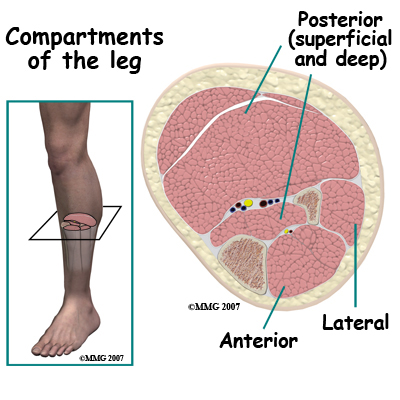
Compartment syndrome occurs when bleeding into the muscle compartments in the leg raises the intra-compartment pressure to levels that slow or stop blood flow in those compartments. Muscles in the leg (and arm, hand and foot) are contained inside compartments bounded by tough inelastic sheets of fibrous tissue. There are four compartments in the leg. The anterior compartment is the soft region in the front outer side of the leg - to the outer side of the shin bone. The lateral compartment is on the outer side and there are two posterior compartments in the calf at the back of the leg.
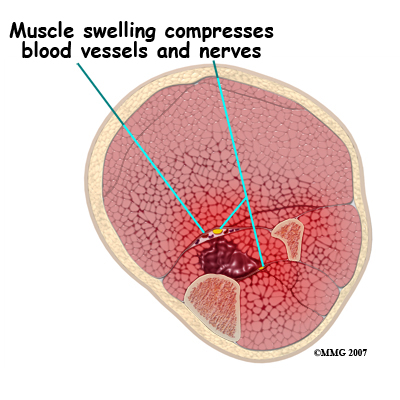
Even quite a small amount of bleeding into one or more of these compartments can cause a problem. This problem can be made worse if the leg is compressed from the outside by a cast or tight dressing. The fundamental problem is that the muscle tissue will die if there is insufficient blood supply. Dying muscle is very painful and unremitting pain is the most reliable sign of a compartment syndrome. However, all fractures are painful and it is sometimes difficult to distinguish between the pain that is normally present after a fracture and the pain of a compartment syndrome. In the latter case the pain is made worse by contracting or stretching the affected muscle; this is one of the reasons the doctors, nurses, and physical therapists insist that patients move their toes, feet and ankles after a fracture.
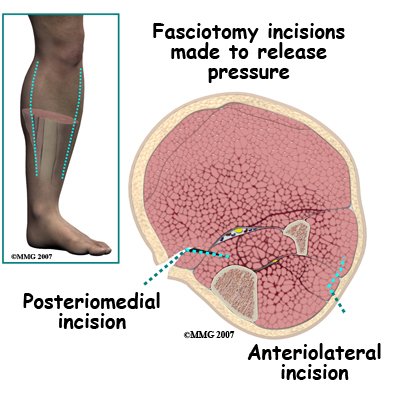
If a compartment syndrome is diagnosed an emergency operation is needed to release the pressure. This is called a fasciotomy and may involve a big opening of the skin of the leg. Once the skin is opened the muscle compartments are also split open and the pressurized contents allowed to bulge out. This relieves the pressure and the blood supply to the muscle can resume. If this procedure is done before any muscle dies the long-term outlook is good, although the wound may require skin grafting and be unsightly. If some muscle death (necrosis) has occurred these parts may shorten up causing contractures and clawing of the toes as well as weakness of the affected muscle.
Chronic exertional compartment syndrome sometimes occurs months or years after the injury. When the patient returns to heavier activities or sports he/she finds that the leg rapidly becomes painful. The pain is made worse by moving the foot or pressure over the muscle and is slowly relieved by resting. This condition can be investigated by measuring the intra-compartment pressures before and after exercise. It is relieved by fasciotomy and the outcome after treatment is usually satisfactory.
Nonunion
 Of all the long limb bones the tibia has the worst reputation for not healing. Nonunion is a clinical diagnosis. It means that in the doctor's opinion, the bone will not heal without further intervention. Delayed union is the state where the bone is taking longer than normal to heal but there is sill a chance it will heal without surgery. Obviously there is an overlap between these two complications as all "nonunions" were "delayed unions" at an earlier point.
Of all the long limb bones the tibia has the worst reputation for not healing. Nonunion is a clinical diagnosis. It means that in the doctor's opinion, the bone will not heal without further intervention. Delayed union is the state where the bone is taking longer than normal to heal but there is sill a chance it will heal without surgery. Obviously there is an overlap between these two complications as all "nonunions" were "delayed unions" at an earlier point.
Clinically, a non-united tibia is found to be painful and to hurt more on bearing weight or on stressing the leg. The pain does not get better with time as occurs with normal healing. Often one cannot feel any movement at the fracture site, but in florid cases one can. The x-ray shows a gap between the fracture fragments and in some cases the formation of a pseudo-joint. It may be necessary to get a CT scan of the region to make sure of the diagnosis. Getting a good image is often made difficult by the presence of metal implants used to treat the fracture.
Treatment of a nonunion is individualized to each different case. Nonunion is more common if the original injury was treated nonoperatively. If surgery has not been undertaken before, the treatment will likely be rigid internal fixation and bone grafting. Bone grafting alone has been used and may be combined with removal of a small section of the fibula if it is thought that the healed fibula is holding the fracture fragments apart. If the fracture has already been operated on the fixation will most likely be replaced with some other system that imposes compression on the fracture site.
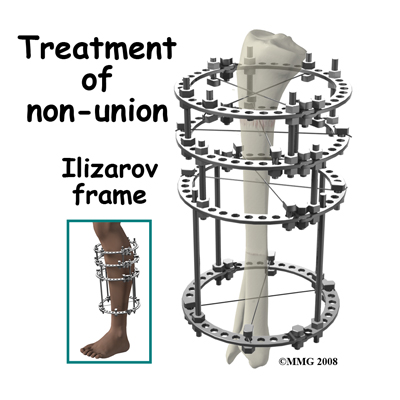
In really difficult cases, the Ilizarov technique may be used. The nonunited segment of bone is removed and freshened ends of normal bone are held together with an external frame. A second cut is made in the normal bone higher up the leg and the frame is used to lengthen the bone over time.
In most cases of nonunion surgery does achieve healing and the long- term outlook is good. Infected nonunion is a particularly difficult problem with a higher failure rate. The main adverse long-term outcome is loss of function caused by the prolonged treatment. If it takes years to heal the bone the muscles and joints of the leg are unlikely to recover fully.
Malunion
If the bone heals in a position that is shortened, angulated, or rotated it may be said to be mal-united. Often this is not a significant problem and does not interfere with long-term function. Studies of malunion have not shown a significant risk of later arthritis of the knee or ankle.
Sometimes the degree of shortening or rotation may not be acceptable. Treatment would then require surgical correction of the malalignment. Surgical correction of a malunion requires cutting the bone, restoring the alignment then fixing the tibia using either internal fixation with a plate, intramedullary rod or external fixation device. These methods are usually successful in correcting the problem and giving a good long-term outcome.
Summary
A fracture of the leg below the knee usually involves both bones of the shin, the tibia and the fibula. Fractures of the tibia are serious injuries which take many months to heal. There is a wide spectrum of injury from simple stable spiral fractures to severe open injuries with bone loss and massive damage to muscle, nerve and blood vessels. In most cases treatment is successful in its aims of saving the patient's life and limb, healing the fracture, and restoring function, but treatment can be prolonged and there are many complications to avoid.
Portions of this document copyright MMG, LLC.