
Kienbock's Disease
|
||||||


Introduction
Physical therapy in Seattle for Wrist
Welcome to Core Physical Therapy's patient resource about Kienbock's Disease.
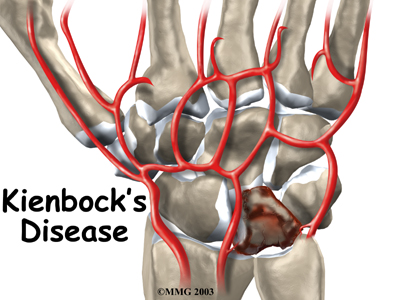
Kienbock's disease is a condition in which one of the small bones of the wrist loses its blood supply and dies, causing pain and stiffness with wrist motion. In the late stages of the disease, the bone collapses, shifting the position of other bones in the wrist. This shifting eventually leads to degenerative changes and osteoarthritis in the joint. While the exact cause of this uncommon disease isn't known, a number of treatment options are available.
This article will help you understand:
- how Kienbock's disease develops
- how doctors diagnose the condition
- what treatment options are available
Anatomy
How does the wrist joint work?
The anatomy of the wrist joint is extremely complex, probably the most complex of all the joints in the body.
Wrist Anatomy
The wrist is actually a collection of many joints and bones. These joints and bones let us use our hands in lots of different ways. The wrist must be extremely mobile to give our hands a full range of motion. At the same time, the wrist must provide the strength for heavy gripping.
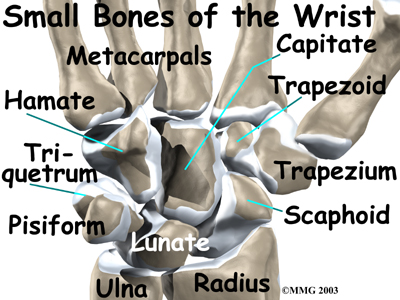
The wrist is made of eight separate small bones, called the carpal bones. The lunate is one of these bones.
It is the bone that is affected in patients with Kienbock's disease.
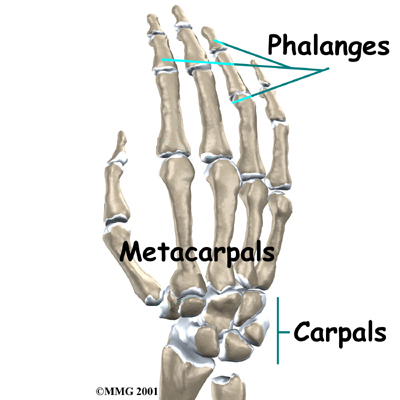
The carpal bones connect the two bones of the forearm, the radius and the ulna, to the bones of the hand. The metacarpal bones are the long bones that lie underneath the palm. The metacarpals attach to the phalanges, which are the bones in the fingers and thumb.
Forearm Bones
Related Document: Core Physical Therapy's to Wrist Anatomy
Causes
Why do I have this condition?
Doctors have not determined exactly what causes Kienbock's disease. A number of factors seem to be involved. Usually the patient has injured the wrist. The injury may be a single incident, such as a sprain, or a repetitive trauma. But the injury alone does not seem to cause the disease.
 The way that blood vessels supply the lunate is thought to play a role in Kienbock's disease. Some bones in the body simply have fewer blood vessels that bring in blood. The lunate is one of those bones. A bone with a limited blood supply may be more at risk of developing the disease after an injury. The reduced blood supply might be the result of a previous injury to the blood vessels.
The way that blood vessels supply the lunate is thought to play a role in Kienbock's disease. Some bones in the body simply have fewer blood vessels that bring in blood. The lunate is one of those bones. A bone with a limited blood supply may be more at risk of developing the disease after an injury. The reduced blood supply might be the result of a previous injury to the blood vessels.
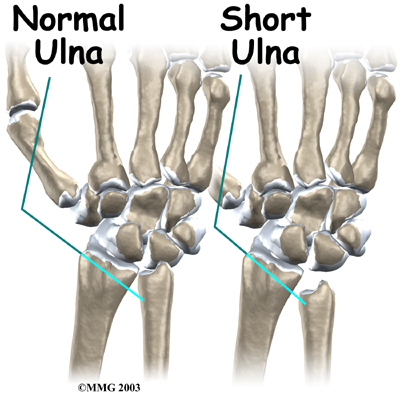
Other bones around the lunate may play a role in the disease, too. The length of the ulna, the bone of the forearm on the opposite side of the thumb, may be a factor. When the ulna is shorter than the radius, an imbalance of pressure is created in the wrist joint. Normally, the ulna supports a portion of the force that needs to be transferred from the hand to the forearm. If the ulna is too short, this cannot occur. The lunate is caught between the capitate bone and the radius and must absorb more force when the hand is used for heavy gripping activities. Over time, this extra force may make it more likely for a person to develop Kienbock's disease. Chronic repetitive trauma can lead to damage of the arteries supplying blood to the lunate.
Kienbock's disease is also sometimes found in people with other medical conditions that are known to damage small blood vessels of the body. Whatever the cause, the lunate bone develops a condition called:
Osteonecrosis
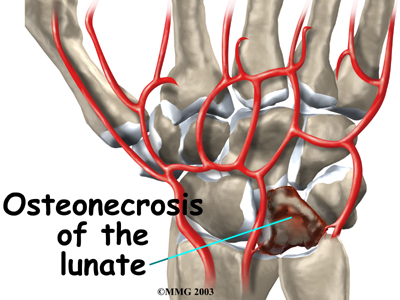
In osteonecrosis, the bone dies, usually because it's not getting enough blood.
Symptoms
What does Kienbock's disease feel like?

The primary symptoms of Kienbock's disease are pain in the wrist and limited wrist motion. Pain may vary from slight discomfort to constant pain. In the early stages there may be pain only during or after heavy activity using the wrist. The pain usually gets slowly worse over many years. The wrist may swell. The area over the back of the wrist near the lunate bone may feel tender. You may not be able to move your wrist as much as normal or grip objects as well.
Patients often have the condition for months or years before seeking treatment. It rarely affects both wrists. Without treatment the bone may collapse. When the lunate bone is displaced or fragmented, it can rub on the tendons that slide along the back of the wrist - the extensor tendons. The abnormal bone may eventually wear through one or more of the extensor tendons along the back of the wrist. The wrist becomes unstable. The resulting misalignment causes even more uneven wear on the bones leading to osteoarthritis between the radius and the carpal bones.
Diagnosis
How do health care providers identify the problem?
When you visit Core Physical Therapy, we will begin by taking a detailed history of the problem and carefully examining your wrist.
Some patients may be referred to a doctor for further diagnosis. Once your diagnostic examination is complete, the physical therapists at Core Physical Therapy have treatment options that will help speed your recovery, so that you can more quickly return to your active lifestyle.
Our Treatment
What can be done for the condition?
Kienbock's disease usually progresses slowly over many years. To help understand it and recommend what treatment is best, the progression of the disease is divided into four stages.
- Stage one: The bone loses its blood supply, and a fracture of the lunate may occur.
- Stage two: The bone hardens (called sclerosis) because of the lack of blood supply.
- Stage three: The dead lunate bone collapses. It may break into several pieces and move out of its normal position.
- Stage four: The surfaces of the nearby wrist bones are damaged, resulting in arthritis of the wrist.
Related Document: Core Physical Therapy's Guide to Osteoarthritis of the Wrist Joint
The goal of physical therapy treatment is to decrease the load across the lunate and/or bring a better blood supply to it. Treatment is determined by what stage the disease is in. Staging can be difficult since the degenerative changes occur slowly over a long period of time. Repeated imaging studies may be needed to confirm earlier suspicious findings.
There is no strong evidence at this time to suggest one treatment works better than another. When you visit Core Physical Therapy, we will look at all the factors and makes the best clinical judgment possible. Your age, occupation, activity level, and findings from the diagnostic process will all be taken into consideration.
Non-surgical Rehabilitation
Stage one Kienbock's disease is usually treated using nonsurgical treatments. Our physical therapist may suggest immobilizing the wrist in a cast for up to three months. It is possible that the blood supply to the lunate will return and the disease will clear up during this time. If the patient has what's known as transient (meaning short-lived) osteonecrosis rather than true Kienbock's disease, the condition may also clear up during this time. Transient osteonecrosis sometimes develops briefly after an injury.
If the bone is in good alignment, your doctor may have your wrist placed in a cast for up to 12 weeks. This amount of time is needed to allow the blood supply to return to the bone. When your doctor is certain the bones have healed, your cast will be removed. Your wrist will probably be stiff and weak from being in the cast. The physical therapy programs offered at Core Physical Therapy can then help improve your wrist range of motion and strength.
Post-surgical Rehabilitation
You'll probably be placed in a splint for about 12 weeks after surgery. Your surgeon will X-ray the wrist several times after surgery to make sure that the bones are healing properly. Once your wrist has begun to heal, you can safely begin our rehabilitation program.
Your first few Core Physical Therapy post-surgical treatments will focus on controlling the pain and swelling. Our physical therapist will have you work into doing exercises to help strengthen and stabilize the muscles around the wrist joint. We may use other exercises to improve fine motor control and dexterity of your hand. Our physical therapist will also give you tips on ways to do your activities while avoiding extra strain on the wrist joint.
At Core Physical Therapy, our goal is to help you keep your pain under control, improve strength, and to regain fine motor abilities with your wrist and hand. When your recovery is well under way, regular visits to our office will end. Although we will continue to be a resource, you'll be in charge of doing your exercises as part of an ongoing home program.
Core Physical Therapy provides services for physical therapy in Seattle.
Physician Review
X-rays and possibly a magnetic resonance imaging (MRI) scan will be ordered. The X-rays are useful to determine how far the disease has advanced. This helps your doctor plan treatment. The MRI machine uses magnetic waves instead of radiation to take a series of pictures that look like slices of the wrist. The MRI scan is most useful if your doctor is not sure whether the lunate bone has lost its blood supply. The MRI is extremely accurate at showing whether a bone has a blood supply or not. Changes in the lunate bone will usually appear on one of these tests. No other tests are usually required.
Surgery
Operative treatment can be broken down into several major categories, including 1) revascularization 2) intercarpal fusion; 3) lunate excision; 4) lunate decompression and joint-leveling procedures; 5) proximal row carpectomy; and 6) wrist fusion.
Revascularization
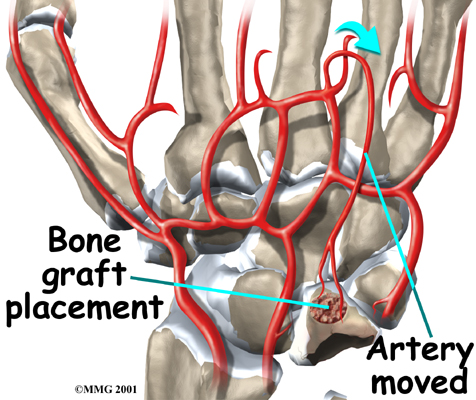 Stage two and stage three Kienbock's disease often require surgery when immobilizing the wrist doesn't help. Attempts to restore the blood flow to the lunate are most likely to be successful when the disease is in the early stages. The procedure to restore blood flow is called revascularization. During the operation, the surgeon moves a small section of blood vessels (and also possibly bone) from elsewhere on the wrist. The segment is attached to the deteriorating lunate bone. This is done to restore blood flow to the lunate and halt its deterioration. This is a newer procedure to treat Kienbock's disease and is not always successful. Vascularized bone graft does have the advantage of implanting live bone with a ready made blood supply.If this is successful, the bone heals and the blood supply in the transferred bone fragment grows into the rest of the lunate to restore the blood supply to the entire lunate.
Stage two and stage three Kienbock's disease often require surgery when immobilizing the wrist doesn't help. Attempts to restore the blood flow to the lunate are most likely to be successful when the disease is in the early stages. The procedure to restore blood flow is called revascularization. During the operation, the surgeon moves a small section of blood vessels (and also possibly bone) from elsewhere on the wrist. The segment is attached to the deteriorating lunate bone. This is done to restore blood flow to the lunate and halt its deterioration. This is a newer procedure to treat Kienbock's disease and is not always successful. Vascularized bone graft does have the advantage of implanting live bone with a ready made blood supply.If this is successful, the bone heals and the blood supply in the transferred bone fragment grows into the rest of the lunate to restore the blood supply to the entire lunate.
Intercarpal Fusion
Using an arthroscope, a thin instrument with a TV camera on the end, surgeons are able to operate using a small incision over the lunate. The surgeon cleans the area around the lunate, and then fuses the lunate to the carpal bone next to it. This is called an intercarpal fusion. It’s not a complete or total fusion because not all of the wrist bones are fused together. Bringing an extra blood vessel to revascularize the lunate (described above) is not necessarily a part of the treatment.
Lunate Excision
One of the oldest methods for treating Kienbock's disease is called a lunate excision. The abnormal bone was just removed, leaving an empty space in the wrist joint. The bones in the area collapsed into the empty space. This usually was not ideal and created problems later on. Other options include filling the empty space with a piece of tendon coiled up and stuffed into the hole. An artificial lunate bone may also be used to fill this space and maintain alignment of the bones.
Lunate Decompression and Joint Leveling
If you were born with an ulna that is too short, you have what is called an ulna minus wrist joint. As described above, this can lead to increased pressure on the lunate and may be contributing to the problem. Your surgeon may recommend a joint leveling procedure to reduce the pressure on the lunate. Doing this may allow the bone to heal and revascularize, or it may at least slow the progression of the arthritis in the joint. A joint leveling operation either shortens the bone that is too long ( the radius) or lengthens the bone that is too short (the ulna). Joint leveling operations include ulnar lengthening and radial shortening osteotomy.
Ulnar Lengthening
The operation for ulnar lengthening is done by making a small incision on the ulnar side of the wrist. The ulna bone is cut. Osteotomy is the term surgeons use to describe cutting a bone. The bone is not cut straight across, but like a stair step. This allows the surgeon to slide the two ends of the bone apart about 1/4 or 1/2 inch and still have the bone overlapping and connected. This type of cut prevents ending up with a large gap between the two segments of bone that can delay or prevent healing.
The surgeon will slide the two segments of ulna apart until X-rays show the joint is level and the radius and ulna are of equal length. The two segments of bone are held in place with a small metal plate and screws until they heal together. The plate may be removed once the bone heals.
Radial Shortening Osteotomy
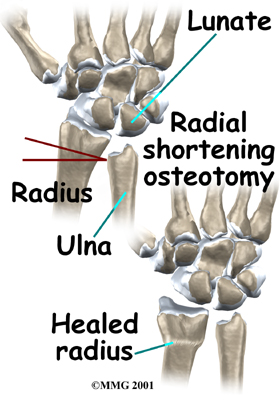
If your surgeon suggests a radial shortening osteotomy, then the goal is to shorten the bone that is too long. A radial osteotomy is sometimes preferred because the bone just heals better. The distal end of the radius near the wrist joint is larger than the ulna with a better blood supply. This means that it heals faster and more reliably.
To perform the radial osteotomy, the surgeon makes a small incision though the skin over the end of the radius. Before the operation, the surgeon uses the X-rays and measures how much bone must be removed to make the joint level. The radius is cut completely in two pieces and a small section, or wedge, of the bone near the wrist is removed. The two segments of the shortened radius are aligned and held in place with a metal plate and screws until healed. Some studies show this method has a lower rate of complications and good outcomes. It is used more often than ulnar lengthening.
 Stage two Kienbock’s disease and wrists in stage three that are stable can be treated with joint leveling procedures. Decreased pain with improved range of motion and strength are possible with joint leveling. But getting the exact length needed can be difficult.
Stage two Kienbock’s disease and wrists in stage three that are stable can be treated with joint leveling procedures. Decreased pain with improved range of motion and strength are possible with joint leveling. But getting the exact length needed can be difficult.
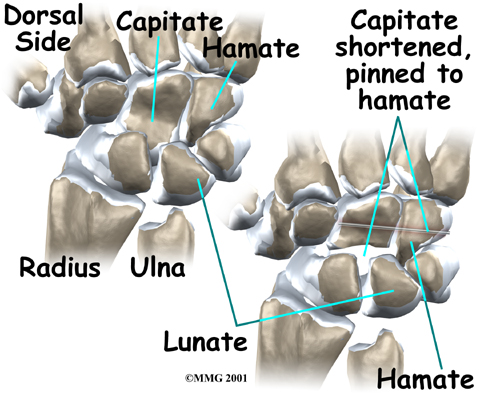
Capitate Shortening
Some surgeons prefer a capitate shortening (known as the Almquist procedure), which shortens a carpal bone on the other side of the lunate. Lunate decompression and capitate shortening are both helpful for reducing the force on the lunate. This procedure does not level the joint.
Carpectomy
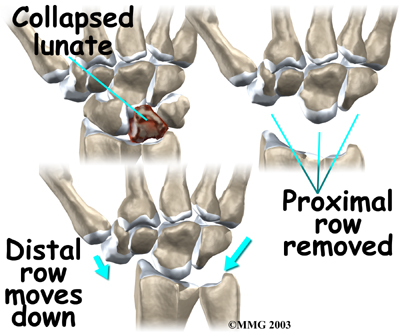
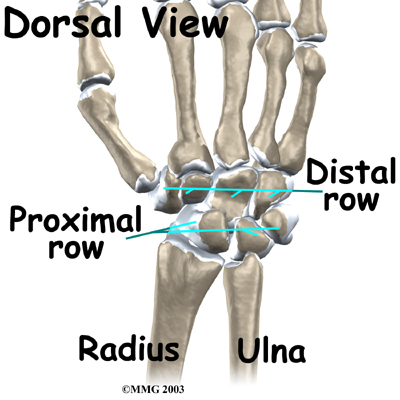
In stage four (late-stage) Kienbock's disease, surgeons focus on treating the wrist osteoarthritis that results when the lunate collapses and dies. One surgical option at this stage is proximal-row carpectomy. Carpectomy means excision (removal) of one or more of the carpal bones. The wrist is made up of two rows of carpal bones, four in each row. The lunate is in the proximal row (the row closest to the forearm). When the lunate has collapsed, but the wrist joint is not terribly arthritic, the four carpal bones of the proximal row may simply be removed. This allows the distal row (the other four bones) to slide down a bit and to begin moving against the forearm bones instead.
The wrist joint seems to work pretty well after this procedure. The advantage is that you will still have a good deal of wrist motion, unlike wrist fusion (described below). A proximal row carpectomy is a good solution when you need a flexible wrist more than you need a strong one, such as in someone who plays piano for a living.
During this procedure, the surgeon can also take out a section of the nerve that supplies feeling to the wrist joint to reduce wrist pain. This will not affect the feeling in your hand, because it only affects the nerve that goes to the wrist joint itself, below the skin level.
Wrist Fusion
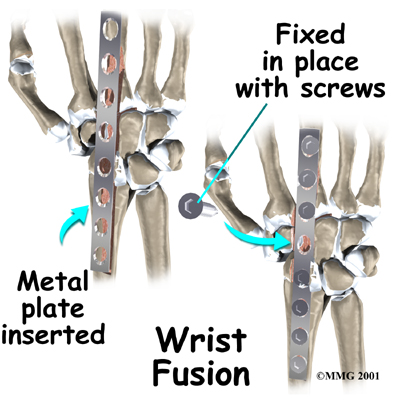
Finally, your surgeon may also suggest a wrist fusion when the entire wrist has become arthritic. (A wrist fusion is sometimes called an arthrodesis of the wrist). A fusion is an operation that allows all the bones of the wrist to grow together to form one bone. This makes the wrist stiff. You will not be able to bend the wrist after a fusion. You will be able to turn the wrist palm up and palm down. A fusion is a good solution when you need a strong wrist more than you need wrist movement, such as someone who does manual labor.
Related Document: Core Physical Therapy's Guide to Wrist Fusion
Portions of this document copyright MMG, LLC.